

at a glance
Inositol Supplements for PCOS: The Ultimate Guide
Table of Contents
- 01 - Inositol and PCOS an Introduction
- 02 - Solutions For PCOS Symptoms and Options to Improve Fertility
- 03 - Weight Loss Recommendations, Supplements and Fertility
- 04 - Insulin Resistance and Hormones with PCOS
- 05 - Higher Insulin Levels Mean Higher Androgen Levels
- 06 - Ways to Decrease Insulin Resistance
- 07 - Metformin or Glucophage: What Your Doctor Has to Offer
- 08 - Myo-Inositol Supplementation for PCOS and PCOS Infertility
- 09 - Why Inositol for PCOS Specifically
- 10 - Inositol and Fertility in PCOS Patients
- 11- Research articles on Myo-inositol and Fertility
- 12- Myo-inositol alone or a 40:1 combination of Myo-inositol to d-chiro inositol?
- 13- Why a 40:1 Ratio of Myo-inositol to D-Chiro Inositol?
- 14- The Research on Inositol and PCOS Evolution
- 15- Different Ratios of DCI comapared to Myo-Inositol Supplementation
- 16- Why I don't Support 40:1 Ratio Formulation Based on This Single Study
- 17- What Type of Inositol Should I take for PCOS?
- 18- Inositol Frequently Asked Questions (FAQ)
- 19- Summary of Inositol Use in PCOS
- 20 - References
- 21 - DISCLAIMER
Inositol and PCOS an Introduction
We are all looking for that magic pill (or in this case powder) to help our PCOS. Myo-Inositol(MI) and its similar-looking friend D-Chiro Inositol(DCI) are promising options in the treatment of PCOS.
Here’s the thing: a lot of people in the influencer world have been promoting a specific product or products with a blend of myo-inositol and d-chiro inositol with a 40 to 1 ratio. This is touted to be a “miracle ratio”.
In my opinion, the scientific literature is not so conclusive as to agree with the “hype”. I want to help you understand why. Let’s dive into some background.
We Need Solutions For PCOS Symptoms and Options to Improve Fertility
PCOS is something that comes with physically frustrating symptoms impacting our self-esteem. What is perhaps just as difficult is the long road ahead for many of us trying to conceive.
PCOS patients struggle with metabolic syndrome, impaired glucose metabolism, decreased ovarian function, higher rates of gestational diabetes, and subfertility. The administration of insulin sensitizers has been shown to drastically improve each of these categories.
As women with PCOS we are constantly looking for solutions both short-term and long term to help manage symptoms, improve our chances at becoming pregnant and decrease the burden of the metabolic consequences that go along with insulin resistance.
If you have PCOS you have likely been told by your doctor to lose weight. Weight loss is the first line of treatment for PCOS because even a small reduction in weight of 5-10% of body weight can restore ovulation and improve our bodies’ abilities to react to the insulin available in our bloodstream. (1)
The problem is losing weight with PCOS is hard! Many PCOS patients have tried with great amounts of effort to lose weight, often with little success or long-term sustainability. We see this in research as well. (2)

While it is difficult to lose weight, the recommendation to do so does have a lot of merit, no matter how frustrating it is to hear. Want to learn more about weight loss and fertility with PCOS, check out this article.
Weight Loss Recommendations, Supplements and Fertility
As a woman with PCOS that struggled with symptoms of weight gain, difficulty losing weight, and infertility I have always looked for what I could do to help my hormones and metabolism.
We see that diet, exercise, sleep support, and stress management can all help in weight loss efforts. Yet – in diving deep into the scientific literature available I was able to find opportunities to support my body in another way: medications and supplements.
Having been in the position of desperately wanting to grow my own family I have seen the predatory behavior that the supplement industry can have with a dedicated and desperate group of individuals.
If there is any chance of pregnancy I have seen women spend thousands of dollars on things like supplements, personal trainers and even see a long list of physicians, acupuncturists, health coaches, dietitians, naturopathic doctors, and ayurvedic healers. The list could go on. Do you relate to this?
It is a difficult landscape to navigate without scientific training on how to evaluate the literature and with the unique struggles we face in the medical landscape as women. I like to call it the “vagina effect”.

It seems if you are in a body with a vagina and have any type of hormonal complaint the answer is hormonal contraceptives(most typically birth control pills). That prescription doesn’t help those of us actively trying to conceive.
We need medical providers to stretch beyond the “vagina effect” and look for the root cause approaches that can meet us in a place aligned with our goals. This is where insulin resistance comes in.
Insulin Resistance and Hormones with PCOS
If you want to learn how insulin resistance can affect the symptoms and hormones in PCOS, check out this article on insulin resistance.
The reader’s digest version is this: 95% of overweight and obese women with PCOS struggle with insulin resistance. (3) We see this number affecting about 75% of women with a BMI under 25, or what the literature terms “Lean PCOS”.
Higher Insulin Levels Mean Higher Androgen Levels
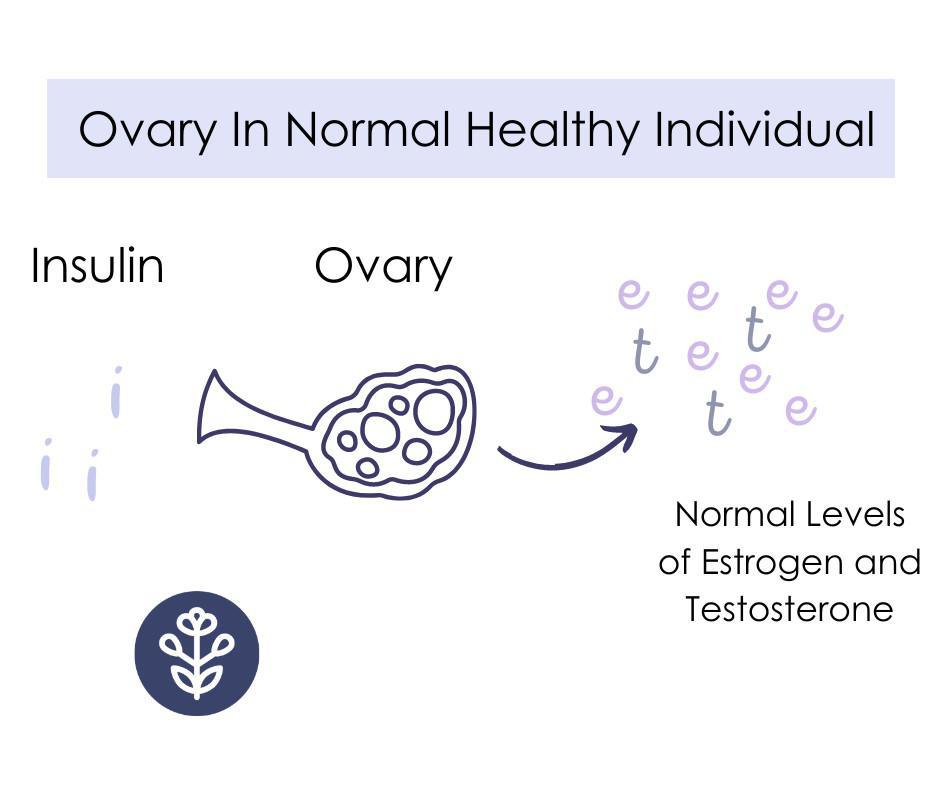
As insulin levels rise in our body the response is nearly a universal resistance to the hormone. I say nearly because our ovaries are an organ that doesn’t become insulin resistant. Thus, high levels of insulin bombard the ovary and the cells within the ovary start becoming mega producers of androgens(aka male hormones).
This is what an ovary looks like when the ovary is exposed to correct amounts of insulin.
In PCOS we have ovaries that have too much insulin exposure leading to over production of testosterone and other androgens. This also happens at the expense of estrogen. This is a problem because estrogen is so important for ovulatory function.
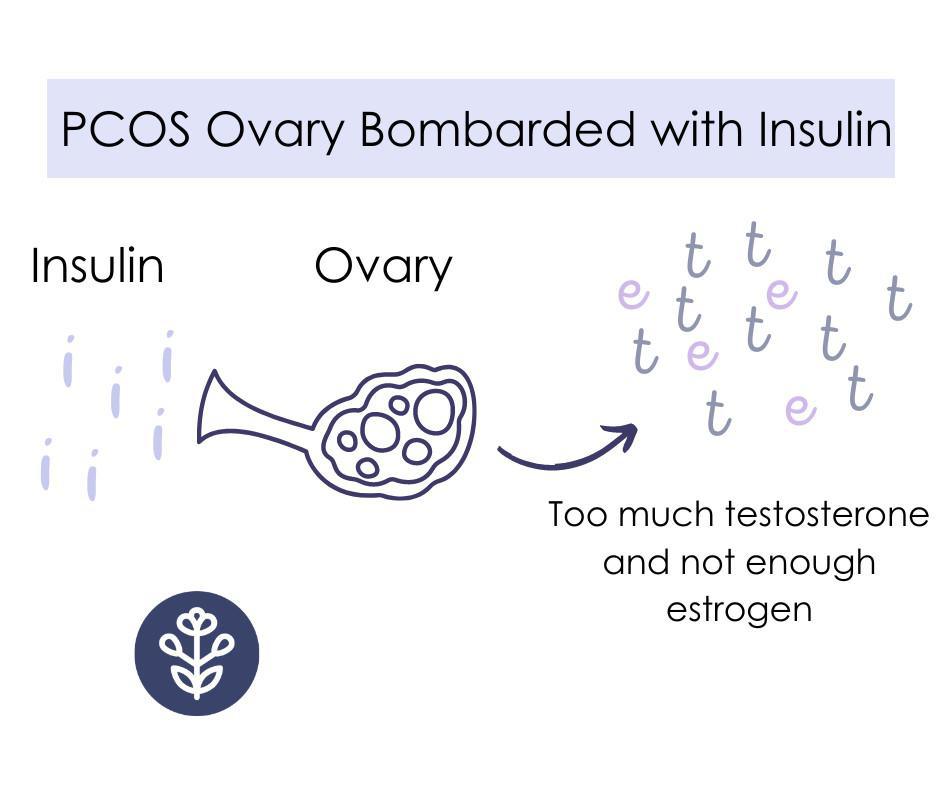
In a more root-cause way to manage this high androgen production, we can target insulin resistance. Less insulin means less of a signal to the ovary, and voila: fewer androgens.
Your Liver and a Protein Called Sex Hormone Binding Globulin Help Lower Insulin Too
There is another way lower insulin levels improve androgen levels. When the liver is exposed to less insulin it can create more of something called Sex Hormone Binding Globulin. Think of this as the thing that floats around bouncing off cells and other things in your blood and when it finds testosterone or DHEA-S it basically turns those hormones off. I like to think of SHBG as the Mrs. PacMan going around gobbling up all the little dots of testosterone.
So if we target insulin resistance we can help make more of Mrs. Pacman and less of the dots for her to eat. See how this could be super helpful?
Ways to Decrease Insulin Resistance
Ready to hear the broken record: diet, exercise, improved sleep and circadian rhythms, weight loss, medications, and supplements.
In this article, we are going to focus specifically on one specific supplements and as we do you’ll see how inositol becomes a great option for PCOS.
Metformin or Glucophage: What Your Doctor Has to Offer
Metformin has a large body of research that shows how it can help in lowering insulin levels. By doing so it also is a promising help in restoring ovulation. Let’s see how.
Metformin, or it’s generic version Glucophage, help lower blood sugar levels by slowing down the liver’s capacity to release sugar into the blood. It makes your liver, muscles, fat and other cells more sensitive to the insulin your body already makes.
It also decreases your body’s ability to absorb all the carbohydrates that you eat. (4) An effective dose of metformin often comes with significant side effects that make it difficult to remain on. It is also a medicine used in an “off label” manner to treat PCOS and I often see doctors prescribing much too low of a dose to make any difference.
Common side effects of metformin include nausea, diarrhea, increased gas, and flatulence (that’s farting). Many of these side effects go away or improve significantly over time. Still many of us can not remain on this medication due to the life-altering side effects.
I lost weight on metformin, not just because of how the medicine primarily works(by lowering insulin resistance), but because of the side effect of feeling so nauseous. I didn’t really want to eat.
We have learned in recent years that it is very metabolically expensive in its use of vitamin B12 and women taking metformin (and birth control for that matter) need to also be supplementing vitamin B12. (5)
While these side effects can change the course of your day they aren’t as scary as other medication side effects like risk of stroke, heart attack, etc. This medication has been used in an “off-label” manner for PCOS for many decades and for good reason.
It helps improve insulin levels, HOMA-IR score, decreases testosterone levels, increases SHBG, and has been shown to help induce ovulation and impact pregnancy rates.
Many choose to take metformin because their medical provider has offered a prescription, it is a relatively inexpensive medication, and often it has very little out-of-pocket expense at all.
I have worked with many women (myself included) who have for one reason or another chosen to discontinue their use of metformin. Many because the side effects were just too troublesome, others because they prefer a more “natural” solution, and others still because in pregnancy they wanted to reduce unnecessary or redundant prescriptions. All of these are valid reasons and should be considered in a patient-centered approach.
When trying to conceive, I found it difficult to continue taking metformin so I dove into the research. My review of the scientific literature led me to a promising alternative: Myo-Inositol.
Myo-Inositol Supplementation for PCOS and PCOS Infertility
Inositol has been the subject of many PCOS conversations and areas of study for years. It is a compound found abundantly in nature. You most likely eat it without even realizing it in foods like fruit, beans, and nuts.

Inositol has 9 different types that we call “stereoisomers”. If the word stereoisomer doesn’t communicate to you – just know it’s like having a favorite shirt that you decided to buy in 9 different colors. Same style, a slightly different look, and effect.
Myo-inositol is the most abundant form found in nature followed by a form called d-chiro inositol. Many scientists have called this a B-vitamin-like substance. I think had it been discovered earlier we would have called it B-26(or something like that).
Our body has the ability to make inositols and inositol isn’t essential to eat for adequate levels to be found in our blood.
Inositol is also similar in taste to sugar alcohols. You have no doubt heard of things like sorbitol, manitol, or xylitol. These are sugar alcohols and have a distinctly sweet taste. You will know if something has a sugar alcohol component because it will have the -itol ending. Myo and d-chiro inositol are no different in that respect – they are sweet-tasting substances.
Why Inositol for PCOS Specifically
What we see with inositols is they function as an alert for the cell to know insulin is around and help signal the cell to do something about it. Myo-inositol specifically acts as a second alert system so the cell knows that energy is available. We like to call it a secondary messenger – it’s not the main alarm or doorbell: that’s insulin.
It’s another avenue of communication though, like an alert you get from Amazon on your phone that a package was just delivered. The delivery driver still rang the doorbell(insulin), maybe you even looked out and saw the UPS truck drive away, but the email comes letting you know that a package is on your doorstep(myo-inositol).
Since inositol helps cells respond to insulin, your body will not have to work as hard to get blood sugar levels within a proper range. Thus it won’t have to create as much insulin.
Remember from earlier:
more insulin > ovaries make >more testosterone
Add inositol to the equation:
inositol > cells respond better to insulin > body makes less insulin > ovary makes less testosterone > symptoms improve/ovulation occurs
Since inositol has been studied for its benefits in PCOS we have seen it affect many areas. It helps both the ovary and muscles/organs to be more sensitive to insulin. Inositol helps lab values improve and symptoms improve.
Labs like testosterone, free testosterone, insulin, and fasting glucose levels have all been reported to go down with inositol supplementation. We have also seen symptoms improve like inducing ovulation and improving cycle length.
We have some evidence and I’ve seen this be the case in many women with PCOS, that it also helps lower cravings for sugar and carbohydrates. Ultimately helping us feel more in control around food. Hallelujah!
Inositol and Fertility in PCOS Patients
There are also studies showing myoinositol, specifically improving egg quality for fertility. In the ovary, we see women with PCOS convert myo-inositol to d-chiro inositol too easily. This impacts the follicle’s production of androgens, increasing them dramatically.
When we look at the follicles of healthy women without PCOS who are also insulin sensitive (the opposite of insulin resistant) there is a ratio of 100: 1 of myo-inositol to d-chiro inositol in the follicular fluid. (6) In other words there is 100 myo to every 1 d-chiro inositol.
In women with PCOS and who are insulin resistant we see a ratio of 0.2:1. (6) Go ahead and read that again. Instead of having 100 myo and 1 d chiro. We have less than 1 myo to every 1 d-chiro. That is a significant difference!
The insulin signaling and testosterone production in the PCOS ovary is just metabolically different.
There are tissues of in the body that have different characteristic ratios of these inositols. Muscles do a very different job than the ovaries do, and they also have different profiles of inositol. Muscles tend to have much more d-chiro inositol as compared to the ovary.
We see this imbalance of ratios in the ovary makes egg quality worse. It also makes ovulation rates worsen.
If you supplement with d-chiro inositol alone we can actually see damaging effects on oocyte quality and ovulation. When supplementing only with myo-inositol – in many research studies we see it has positive effects: lowering androgens, increasing ovulation, and increasing progesterone production.
Research articles on Myo-inositol and Fertility
Research articles on Myo-inositol and Fertility
What we have learned over time is that myoinositol is very helpful for oocyte (or baby follicles/eggs) quality. We have seen in women undergoing IVF that supplemented with 4 gm of myoinositol daily with 400 micrograms of folic acid improved IVF outcomes. (7)
Myo-inositol decreases the risk of Gestational Diabetes(GD) in pregnancy. This is important for this population specifically because PCOS alone increases the risk of GD.(8)
Myo-inositol alone or a 40:1 combination of Myo-inositol to d-chiro inositol?
This is the million-dollar question!
Early on in the study of inositols for PCOS there was a significant understanding that supplementation with high doses of d-chiro inositol actually had negative metabolic effects too.
It was found in early PCOS research that women with polycystic ovary syndrome excreted too much d-chiro inositol in their urine. This was interesting to researchers, so the conclusion was that women with PCOS might need more d-chiro inositol because they were getting rid of too much of it via urine.
Well, this ended up back-firing. Supplementation of d-chiro inositol alone was shown to actually decrease ovulation, not increase ovulation rates. As researchers continued to consider this it was found that women with PCOS have ovaries that are hyperactive in the conversation of myo-inositol to d-chiro inositol.
Peeing out extra d-chiro inositol wasn’t because PCOS gals were making too little of it, they were actually making too much of it.
Since then researchers have sought to find out what ratio of inositol supplementation could have the best impact on PCOS symptoms, lab markers, ovulation, and pregnancy rates.
In the past 3-4 years I have seen vast numbers of medical doctors and influencers recommend a combination of myo-inositol and d-chiro inositol at a 40:1 ratio. Let’s see why…
Why a 40:1 Ratio of Myo-inositol to D-Chiro Inositol?
Okay lady, it's about to be super sciencey in here. If you don't want to trudge through the nuance, skip to the end of this section for the bold print.
Myo-inositol and d-chiro inositol have two different jobs when it comes to glucose.
Myo-inositol: helps cells take in blood sugar. (10)
D-chiro inositol: helps cells turn sugar into a stored form for later: glycogen. This happens to a great degree in the muscle cells and liver cells. (10)
Now in the context of the ovary cells, the two different forms have different jobs as well.
Myo-inositol: helps ovaries to be sensitive to FSH(10)
D-chiro inositol: causes ovaries to make too much testosterone and stop testosterone from turning into estrogen (10)
Taking in energy(myo-inositol) and helping store that energy efficiently for later (d-chiro inositol) are both very important jobs. Since different muscles, tissues, and organs in the body have different jobs, it makes sense they would have different concentrations of these two forms of inositol.
Muscle tissue, adipose tissue, and the liver all store energy for later use and require more d-chiro inositol.
Tissues with high glucose consumption but, less of a need to store it have less d-chiro inositol: brain, heart, and you guessed it: the ovaries!
In the PCOS ovary compared to someone without PCOS - myo-inositol turns into d-chiro inositol too readily. Meaning: too much d-chiro and not enough myo. This is a problem because more d-chiro inositol means more testosterone, less estrogen, less receptive to follicle-stimulating hormones.
Once myo-inositol becomes d-chiro inositol it can not convert back.
So how has the research on inositol and PCOS evolved to where we are today?
In early PCOS research, they gave a lot of d-chiro inositol because so much was being urinated out, they thought these women needed more. What they didn't know then, was more was being urinated out of the body, because too much was being made in the ovary.
So why the 40:1 ratio? Remember how the different tissues had different ratios of these molecules? Well, the plasma (or blood) ratio is 40:1. So researchers started with mice who were induced to have PCOS and tried out different ratios and the ratio of 40:1 had the greatest impact.
Considering that different tissues have different physiological ratios of these stereoisomers, it made sense to test the ratio most often present in the blood.
Once seeing the results in mice, researchers turned to clinical trials in humans. There is one main study that is often cited when comparing myoinositol and d-chiro inositol.
Different ratios of d-chiro inositol compared to myo-inositol supplementation
The one study I see cited most often is this study: Nordio, M et al. “The 40:1 myo-inositol/D-chiro-inositol plasma ratio is able to restore ovulation in PCOS patients: comparison with other ratios.”
In the study fifty-six PCOS patients were divided into 7 different groups with 8 participants each. The cohorts were administered a different ratio of myo-inositol to d-chiro inositol. The ratios were:
- DCI alone
- 1 MI:3.5 DCI
- 2.5 MI:1 DCI
- 5 MI:1 DCI
- 20 MI:1 DCI
- 40 MI:1 DCI
- 80 MI:1 DCI
The total dosage was 2 gm of inositol twice daily for 3 months. They looked at multiple outcomes: ovulation, improvement in FSH, LH, Sex Hormone Binding Globulin (SHBG), 17-beta-Estradiol (E2), free testosterone, before and after meal insulin levels, as well as HOMA index, BMI, and menstrual cycle bleeds.
Per the study, the results were this:
Results: We found that the 40:1 MI/DCI ratio is the best for PCOS therapy aimed at restoring ovulation and normalizing important parameters in these patients. The other formulations were less effective. In particular, a decreased activity was observed when the 40:1 ratio was modified in favor of DCI.
Conclusions: Our data demonstrated that DCI activity is beneficial mainly at a specific ratio with MI, whereas the increase of DCI causes the loss of the beneficial effects at the reproductive level. These results in humans validate a previous preclinical study with different MI/DCI ratios carried out in an experimental model of PCOS mice.
Research is never perfect, but there are considerable issues I see with the above results and conclusions.
Why I can’t support this 40:1 miracle formulation based on this study
While the purpose of the study was to see what the best ratio of d-chiro to myo-inositol is. The study design considered various different ratios including a sample of women who only received d-chiro inositol. Surprisingly they didn’t test only myoinositol.
This is exceedingly difficult in my opinion to draw a conclusion that 40:1 is the best ratio when prior to this study it was already generally known that d-chiro inositol on its own was detrimental to ovulatory function. Myo-inositol administered on its own was already widely recognized in the community to be helpful for both metabolic parameters AND improving ovulatory function.
I’m left really scratching my head wondering why in this study they didn’t want to test the idea that myo-inositol alone, 100:0 MI/DCI wasn’t worth comparing.
Aside from the study design when I look at the group’s pre-study insulin levels before and after meals, the group that received the 40:1 ratio had higher pre and post-meal numbers than the 80:1 group. Improving insulin resistance would help with clinical outcomes like ovulation. We would expect to see improvements in this group as they had more need for improvements.
There are three other major issues with this study.
- The sample size
- The length of inositol administration and data collection
- We have no idea if any of the groups had major dietary or exercise level changes over the course of 3 months
It doesn’t take a data scientist to realize 8 people in each sample group is a small number. It would be hard to make any sweeping claims off such a small study. Yet, in the PCOS community people are taking this 40:1 ratio like it’s dogma and any other formulation steals your ticket to heaven.
In almost any other clinical trial (with big money behind it), they would test in much larger cohorts for a longer period of time.
Now, time is an interesting consideration. It takes 90-100 days to make a “baby egg” grow to mature to the point of ovulation. So taking supplements for 3 months is truly a short period of time to take something to draw ovulatory and pregnancy outcomes regarding.
Finally, we know studies don’t happen in a vacuum. One group could have inadvertently made other positive or negative changes to make their body more insulin sensitive which would have also impacted lab values tracked or outcomes like ovulation and pregnancy.
Perhaps the most disturbing revelation when reading this study on it’s own was that inclusion criteria did not require someone to be anovulatory. You could potentially have a diagnosis of PCOS without struggling with ovulation. Thus the 40:1 group could have included women with PCOS that already were ovulating regularly or more of whom were ovulating compared to other cohorts in the study.
They did require someone to have struggled with fertility for 1 year or more OR to be anovulatory. Yet, you could struggle to get pregnant while ovulating at some frequency. This is a major flaw in this study design.
Overall the sweeping conclusion I can make from this study is we see inositol is beneficial for many metabolic parameters and that the ratios where d-chiro inositol is administered in a smaller ratio to myo-inositol favor reproductive health. Honestly, this isn’t surprising based on what we have known about how the two molecules affect hormones and signaling in the ovary and follicle itself.
Could 40:1 be a good ratio, especially as this is the ratio we find in serum levels? Yes, it can be and is. Is it the best and only ratio that should be administered? I have many doubts about that and think answering that question necessitates further study.
If you spend any time on social media in the PCOS pages you will find many influencers and practitioners recommending 1 or 2 major brands of inositol products and by and large these brands are using this miraculous 40:1 ratio.
Here are some brief thoughts on what to consider for yourself.
What type of inositol should you take for your polycystic ovary syndrome(PCOS)?
What inositol should you take for your polycystic ovary syndrome?
Have you taken a blend of 40:1, was it helpful? Did it restore ovulation for you, help with sugar cravings? Potentially you should continue that.
Have you tried myoinositol alone instead of just the 40:1? It is typically much less expensive per serving and works just as well.
I am typing that as a practitioner that has now treated thousands of women with PCOS. I have worked with many women coming to me to improve fertility and switch them from a 40:1 ratio to myo-inositol only and often see improvements and ovulation occur.
Much of the research doesn’t necessarily focus on these ratios as much as myo-inositol being exceptionally helpful, and if you are trying to get pregnant, it’s my opinion we shouldn’t give you any more d-chiro inositol.
Your ovary is already doing a great job of making that form. The overproduction of d-chiro inositol is causing too much testosterone and impacting your PCOS and ovulation.
You don’t need any more d-chiro inositol if you are trying to get pregnant, you need more myo-inositol.
I bet you have lots of other questions, let’s answer some of the most common ones:
INOSITOL FAQ (Frequently Asked Questions)
Who should consider inositol supplementation?
If you have PCOS you should consider trialing inositol supplementation. This is true no matter your health goals. I have seen it reduce sugar cravings, lower appetite, improve ovulation, decrease androgenic symptoms like hirsutism and hair loss – among other positive things. It’s worth a try. It’s readily available, relatively inexpensive and could really help!
How much inositol should I take in a day?
Most of the research supports a dose of 4 gm per day. Inositol is a supplement that typically comes in powder form for a few reasons. It tastes sweet and most people have no problem adding it to a food or drink. It is also a pretty large dose: 4 gm. So taking that in capsule form usually means taking 7-9 capsules, and that is a lot.
Are there side effects to taking inositol?
Usually, side effects are minimal. Some people will report loose stools for a few days. This isn’t very common, and in all my years of experience, this is typically more of an issue with metformin than with inositol.
Should I take myo-inositol or metformin?
As the market shifts to wanting more natural solutions that have less side effects choosing myo-inositol seems like a no-brainer. When you put these two options up against one another what do we see? Can myo-inositol actually be a substitute and is there reason to consider it even before metformin?
There was a meta-analysis where multiple studies were considered that included a total of 355 women with PCOS.(9) There were similar results with patients who took myo-inositol compared to metformin. Both treatments provided improved insulin sensitivity and lowered testosterone levels. After seeing many hundreds of patients on both of these I have seen similar things in practice. Both have the capacity to help. Myo-inositol has much less reported side effects and tends to also improve egg quality.
This question really is “should I take both?” Should I take myo inositol AND metformin?
I have often started working with individuals that are already on metformin. Instead of switching to myo-inositol we consider adding myo-inositol on top of metformin.
Why?
There was a study published in 2019 that evaluated the synergistic effect of both metformin and myo-inositol versus metformin alone. (13) The group that received the combination had more improvement in menstrual cycle length, bleeding days, and hormone levels.
Perhaps the most important statistic was that the group that took both metformin and myo-inositol had a significantly higher live birth rate. That’s what we are after anyways, right? Babies!
The group that had both metformin and myo-inositol had a live birth rate of 55% that was 33 out of 60 participants versus the metformin alone (16 out of 60 participants).

Look at this sweet family who was a part of my Find Fertility course and got this type of intervention-based care! Look at their sweet son!
Just remember: When adding in any new supplements it’s always good to loop in your practitioners. There is an overlap in how this supplement and metformin work in terms of insulin sensitivity. So be sure to also keep snacks around in case you have a low blood sugar event.
Inositol has additional benefits with regards to egg quality that metformin does not and for that reason is often a good option to layer in over metformin if fertility is a concern for an individual. (12)
In studies both 40:1 and myo-inositol work just as well as metformin improving insulin sensitivity and improving ovulation rates. This is great because we have both pharmaceutical (metformin) and supplement/over-the-counter (inositol) options.
Should I stop taking inositol when I get pregnant?
NO! Of course, always check with your own licensed medical provider – reading this blog does not constitute as medical advice. Inositol can help with managing insulin resistance in pregnancy, which is something that occurs naturally. Unfortunately, those of us entering pregnancy with insulin resistance from PCOS have an increased risk of gestational diabetes, so staying on myo-inositol can be very helpful.
Can inositol help with gestational diabetes?
When considering evidence-based decisions this is one area we do have research for myo-inositol, but we don’t have research for 40:1 ratio to help treat gestational diabetes. Consider just buying myo-inositol if you have this diagnosis. (12)
In fact, not only can myo-inositol help treat, but it can also help prevent gestational diabetes in PCOS women.
Should I take it with food?
I typically recommend taking 15-20 minutes before a meal and taking it twice daily. Your inositol will compete for absorption in the GI tract with other carbohydrates, so taking it before a meal will ensure you optimally absorb your dosage.
Can inositol supplementation help someone that doesn’t struggle with insulin resistance?
Inositol supplementation can help individuals that don’t have insulin resistance because there is still a pathway in the ovary that over-converts myo into d-chiro inositol. Remember how the d-chiro form up-regulates testosterone production? For that reason alone, it is worth considering even if an individual doesn’t struggle with insulin resistance.(15)
Can inositol supplementation help if you have lean PCOS?
Inositol supplementation has been shown in research to help support individuals with a “normal” BMI or those in the overweight or obese categories. (15)
Inositol can be helpful for PCOS individuals especially when combined with diet, and other lifestyle factors.
Summary of Inositol Use and PCOS
No supplement alone should be considered the “fix” for PCOS. This is one supplement that has a lot of promise in its administration. It’s widely recognized that taking too much of the d-chiro form of inositol can be counterproductive for symptom resolution, ovulation, and pregnancy rates.
Taking myoinositol alone and in the form of 40:1 myo to d-chiro form can be helpful for fertility. We need more research as to which form would be best while stimulating ovulation.
Many studies consider other supplemental vitamins or compounds in combination with inositol which can further improve outcomes. Most commonly it is combined with folate or folic acid.
I typically recommend a 4 gm dosage of myo-inositol in combination with diet and other lifestyle modifications.
We have three products in the PCOS Formularies line that contain myo-inostiol. The first is Myoinositol Plus and the second is Metabolic Ovary Formula and the third is Anti-Oxidant Ovary Formula.
The Metabolic Ovary Formula also has other insulin-sensitizing ingredients like chromium, magnesium, and NAC. It also focuses on lowering inflammation, improving egg quality, and other metabolic factors with the addition of CoQ10 and turmeric.

Myoinositol Plus includes support for relaxation, lowering anxiety, and improving sleep quality and can be a formula to take at night.

Anti-Oxidant Ovary Formula is specifically designed with additional antioxidants and some vitex to help boost egg quality and progesterone levels after your luteal phase.
Each contains a 2 gm dose of inositol. Ideally you would pick two of the products to get to the 4 gm dose. You can take all 3 daily if needed and focusing on egg quality and trying to stimulate ovulation.
As a dietitian, PCOS patient, and mother to girls more likely to develop PCOS, I will always have myo-inositol in my medicine cabinet. Actually, it typically lives on my kitchen counter so I remember to take it.
DISCLAIMER
The advice provided in this article is for informational purposes only. It is not meant to augment and not replace consultation with a licensed health care provider. Consultation with a physician, dietitian, naturopathic doctor or other primary care provider is recommended for anyone suffering from a health problem.

I’M CAITLIN JOHNSON!
You are ready to trust your body again. You are ready to fix your hormones and fall in love with your body. Let me show you the way through comprehensive courses to manage your hormones and boost your fertility with PCOS.
Are you
struggling to get pregnant and you don’t know what step to take next. Join Find Fertility today and discover the process hundreds have used to get pregnant and have their dream baby.












